
When your liver gets scarred, it doesn’t bounce back like a bruise. Once cirrhosis sets in, the damage is permanent. This isn’t just about feeling tired or having a funny stomach. It’s about your liver slowly losing its ability to do the jobs that keep you alive - cleaning your blood, making proteins, digesting food, and stopping you from bleeding out from a tiny cut. And if it keeps getting worse, you could end up needing a new liver.
What Exactly Is Cirrhosis?
Cirrhosis is the end result of long-term liver damage. Think of your liver as a factory. When it’s healthy, it’s full of soft, working cells. But when something keeps hurting it - like years of heavy drinking, hepatitis, or too much fat in the liver - those cells die and get replaced with tough, inflexible scar tissue. This scar doesn’t work. It doesn’t filter toxins. It doesn’t make bile. It just sits there, blocking blood flow and crushing the healthy tissue around it.
The term comes from the Greek word kirrhos, meaning tawny yellow - the color a damaged liver turns. But you won’t see it. You won’t feel it at first. That’s the dangerous part. Many people don’t know they have cirrhosis until it’s too late. By then, the liver is already struggling to keep up.
Compensated vs. Decompensated: The Two Stages
Not all cirrhosis is the same. There are two stages, and the difference between them can mean the difference between living a normal life and fighting for survival.
Compensated cirrhosis means your liver is scarred, but it’s still managing to do the basics. You might feel fine. You might not even know you have it. Blood tests might show slightly high liver enzymes or low platelets. But you can still work, eat, sleep, and go about your life. The problem? This stage can last years - or it can crash suddenly. There’s no warning.
Decompensated cirrhosis is when the liver finally gives out. This is when symptoms hit hard: your belly swells with fluid (ascites), your hands shake or you get confused (hepatic encephalopathy), you vomit blood from burst veins in your esophagus (variceal bleeding), or your skin and eyes turn yellow (jaundice). At this point, your liver isn’t just damaged - it’s failing. Survival rates drop dramatically. Without a transplant, many won’t make it past a year.
What Causes It?
Cirrhosis doesn’t come out of nowhere. It’s the result of years of abuse or disease. The big culprits today are:
- Alcohol: More than 3 drinks a day for men, 2 for women, over years. This is still one of the top causes.
- Non-alcoholic fatty liver disease (NAFLD): This is now the fastest-growing cause. It’s linked to obesity, diabetes, and high cholesterol. You don’t even have to drink to get it.
- Hepatitis B and C: Especially hepatitis C. Before modern treatments, it was the #1 reason people ended up on transplant lists. Now, with new antiviral drugs, many can be cured before cirrhosis develops.
- Autoimmune diseases: Like autoimmune hepatitis or primary biliary cholangitis, where your immune system attacks your own liver.
- Genetic conditions: Hemochromatosis (too much iron), Wilson’s disease (too much copper), or alpha-1 antitrypsin deficiency.
Here’s the thing: if you catch it early - before scarring becomes widespread - you can often stop or slow it. Quit drinking. Lose weight. Get treated for hepatitis. But once cirrhosis is full-blown, you can’t undo the scars. That’s why early detection matters more than anything.
How Is It Diagnosed?
You won’t find cirrhosis with a quick checkup. Doctors look for it in layers.
- Blood tests: Look for high bilirubin (yellow pigment), low albumin (a protein your liver makes), high INR (a clotting time), and low platelets (often under 150,000). These aren’t normal values - they’re red flags.
- Imaging: Ultrasound, CT, or MRI can show a shrunken, lumpy liver. But the real game-changer is elastography. This non-invasive scan measures liver stiffness. A reading over 12.5 kPa strongly suggests cirrhosis. It’s replacing biopsies in most cases.
- Biopsy: Still the gold standard, but only used if other tests are unclear. A tiny piece of liver is pulled out and looked at under a microscope. You’ll see the classic pattern: nodules of healthy tissue surrounded by thick scar bands.
Doctors also use scoring systems to measure how bad it is:
- Child-Pugh score: Uses bilirubin, albumin, INR, ascites, and brain function. Scores A, B, or C tell you your 1-year survival chances - 100%, 80%, or 45%.
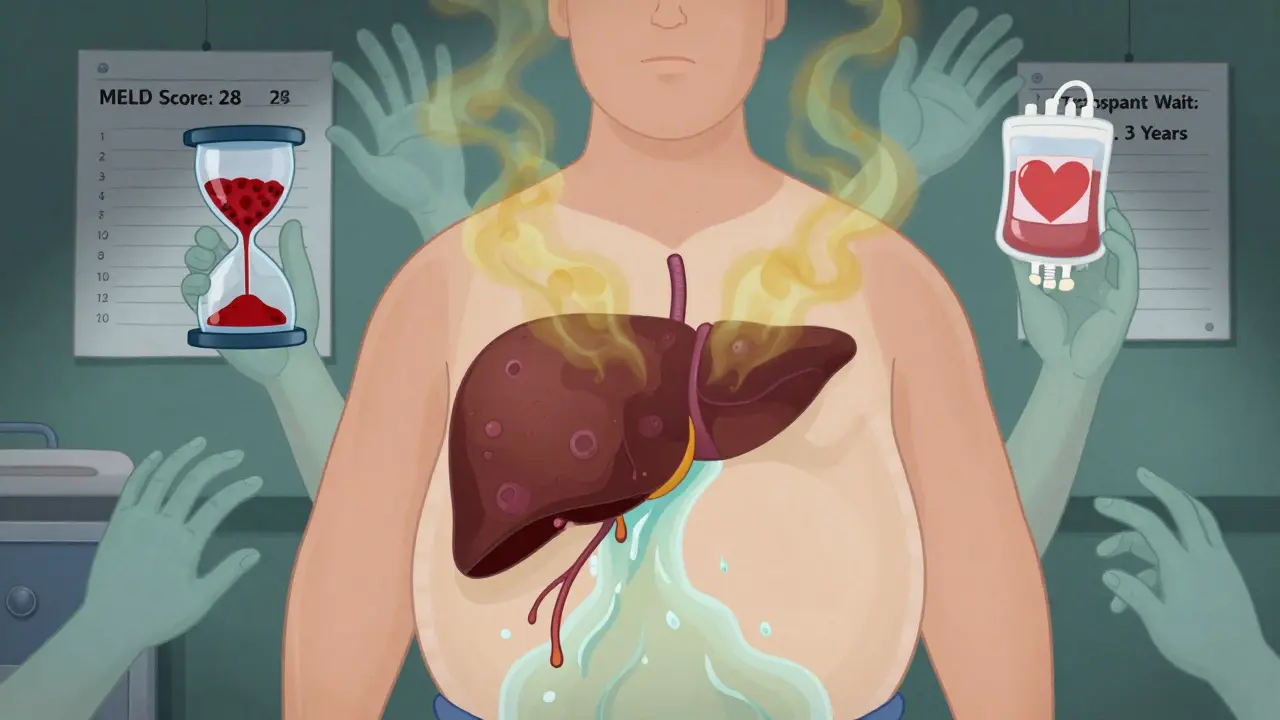
- MELD score: Used for transplant priority. It’s based on bilirubin, creatinine, and INR. Higher score = sicker = higher on the transplant list. A score above 15 means you’re at serious risk of dying without a transplant.
What Happens When the Liver Fails?
When cirrhosis turns to liver failure, your body starts shutting down. Here’s what you’re up against:
- Ascites: Fluid builds up in your belly. It’s painful. It makes breathing hard. It can get infected (spontaneous bacterial peritonitis), which is deadly if not treated fast.
- Hepatic encephalopathy: Your liver can’t clean ammonia from your blood. It builds up and messes with your brain. You get confused, forgetful, sleepy, or even comatose. You might smell sweet or musty. It’s terrifying - and reversible if caught early.
- Bleeding: Scar tissue blocks blood flow, causing pressure to build in the portal vein. This forces blood into fragile veins in your esophagus and stomach. They swell, then burst. Bleeding can be sudden, massive, and fatal.
- Infections: Your immune system weakens. You get pneumonia, urinary infections, or sepsis more easily.
- Liver cancer: Cirrhosis is the biggest risk factor for hepatocellular carcinoma. About 1 in 3 people with cirrhosis will develop it.
These aren’t just complications. They’re life-threatening emergencies. And once one happens, others are likely to follow.
Liver Transplantation: The Only Cure
If you’re in decompensated cirrhosis, a transplant is your only real chance. It’s not a cure-all - it’s a second chance.
Here’s how it works:
- You’re put on a waiting list based on your MELD score. Higher score = higher priority. The average wait in the U.S. is 3 to 5 years. But 12% of people on the list die before a liver becomes available.
- Donors are usually people who died suddenly - brain dead, with healthy organs. Living donors are rare and only used in specific cases.
- After transplant, you’ll need lifelong immunosuppressants. These drugs stop your body from rejecting the new liver. But they also make you more vulnerable to infections and cancer.
- Survival rates are good: 85% of patients live at least 5 years after transplant. Some live 20+ years.
But not everyone qualifies. You have to be healthy enough to survive surgery. No active alcohol or drug use. No uncontrolled infections. No advanced cancer. And you have to be willing to change your life forever - no more drinking, no more smoking, strict diet, daily meds, regular checkups.
Can Cirrhosis Be Reversed?
Here’s the hard truth: once cirrhosis is established, you can’t undo the scarring. No pill, no diet, no supplement can bring back dead liver cells. That’s why prevention and early intervention are everything.
But there’s hope. If you catch it in the compensated stage - and you remove the cause - your liver can improve. Studies show that people who stop drinking, lose weight, or cure hepatitis C can see fibrosis shrink. Some even move from cirrhosis back to mild fibrosis. It’s rare, but it happens. It’s not magic. It’s biology. Your liver is tough. It just needs a chance.
Living With Cirrhosis
If you have cirrhosis, your life changes. Not because you’re sick - but because you have to be smart.
- Sodium: Less than 2,000 mg a day. No processed food. No canned soup. No soy sauce. Water retention is your enemy.
- Protein: You need it - but too much can trigger encephalopathy. Work with a dietitian. Not all protein is equal. Plant-based and dairy are often safer than red meat.
- Medications: Your liver can’t process drugs like it used to. Even Tylenol can be dangerous. Always check with your doctor before taking anything - even herbs or vitamins.
- Monitoring: Blood tests every 3-6 months. Ultrasounds for liver cancer every 6 months. Watch for swelling, confusion, or dark urine. Call your doctor immediately if something feels off.
Support matters. Join a patient group. Talk to a liver nurse. The American Liver Foundation offers free nurse navigation (1-800-GO-LIVER). You’re not alone.
The Future: What’s Next?
Science is moving fast. New drugs are being tested to stop or reverse scarring. One, called simtuzumab, showed a 30% slowdown in fibrosis in early trials. Non-invasive scans are getting smarter - MRI elastography now catches cirrhosis with 90% accuracy.
Transplant tech is improving too. Machines that keep donor livers alive outside the body (normothermic perfusion) are increasing the number of usable organs by 22%. And researchers are testing lab-grown liver cells. One trial showed a 40% drop in MELD scores after injecting healthy liver cells into patients.
But the biggest challenge remains: not enough organs. In the U.S., there are 14,300 people waiting. Only 8,780 transplants were done in 2022. That gap is growing. Until we solve that, prevention - stopping cirrhosis before it starts - is the most powerful tool we have.
Can you live a normal life with cirrhosis?
Yes - if it’s caught early and the cause is removed. Many people with compensated cirrhosis live for years without symptoms. But you must avoid alcohol, eat low-sodium food, take prescribed meds, and get regular checkups. Once decompensation starts, life becomes much harder. Transplant is the only way back to normal.
Is cirrhosis the same as liver cancer?
No. Cirrhosis is scarring. Liver cancer is a tumor. But cirrhosis is the #1 risk factor for liver cancer. About 1 in 3 people with cirrhosis will develop it. That’s why everyone with cirrhosis gets an ultrasound every 6 months - to catch cancer early, when it’s still treatable.
Can you get a liver transplant if you used to drink?
Yes - but only if you’ve been sober for at least 6 months. Most transplant centers require proof of sobriety, counseling, and support systems. It’s not about punishment. It’s about survival. If you go back to drinking after a transplant, you’ll likely lose the new liver.
Are there any drugs that cure cirrhosis?
No. There’s no drug that reverses established cirrhosis. Some drugs, like obeticholic acid, help slow progression in specific types (like primary biliary cholangitis). But they don’t remove scar tissue. The only way to restore function is through a transplant - or by stopping the damage early.
How do you know if your cirrhosis is getting worse?
Watch for swelling in your belly or legs, confusion or memory loss, yellowing of skin or eyes, vomiting blood, or black, tarry stools. These are red flags. Call your doctor immediately. Blood tests and imaging will confirm if you’ve moved from compensated to decompensated cirrhosis.
One thing is clear: cirrhosis doesn’t care how old you are, how much money you have, or how healthy you think you are. It creeps in silently. But if you know the signs - and act fast - you can still beat it. The liver is resilient. It just needs you to listen.



Reviews
Reading this made me think of my aunt. She was diagnosed with compensated cirrhosis five years ago after a routine blood test showed low platelets. No symptoms, no warning. She quit drinking cold turkey, started eating nothing but home-cooked meals, and lost 60 pounds. Last year, her elastography reading dropped from 18.2 to 9.1 kPa. Her doctor said it was the first time he’d seen fibrosis reverse like that. It’s not magic-it’s biology, like the post said. Her liver didn’t heal because of pills. It healed because she stopped destroying it. I wish more people understood that the cure isn’t in a pharmacy-it’s in the choices you make every day.
It’s scary how many people think ‘I’m not an alcoholic’ means they’re safe. Two drinks a night, every night, for 15 years? That’s not social drinking. That’s slow suicide with a side of denial.
I’m not judging. I’m just saying: if you’re reading this, maybe you’re one step away from being the next statistic. And you don’t have to be.
Also, NAFLD is a silent epidemic. No one talks about it because it’s ‘your fault.’ But the truth is, we live in a world built around sugar, stress, and sedentary jobs. Blaming individuals without changing systems is just cruelty disguised as responsibility.
India has the highest number of fatty liver cases in Asia. No one talks about it. Everyone thinks alcohol is the only cause. My cousin got diagnosed at 32-never drank. Just ate biryani daily, worked 12-hour shifts, slept on the couch. Now he’s on the transplant list. We need awareness here. Not just in the US.
Also, why is no one talking about how cheap liver transplants are in India? 30k USD vs 500k in the US? We have world-class hospitals. But no one knows because the system doesn’t promote it. Shame.
Man, this post is a masterclass. I’ve been a nurse for 18 years and I still learned a few things. The part about elastography replacing biopsies? That’s huge. I’ve seen people terrified of liver biopsies-pain, risk, recovery. Non-invasive scans are a game-changer.
Also, the 6-month sobriety rule for transplants? Totally fair. I’ve seen people get transplants, go back to drinking, and lose the liver in 11 months. It’s heartbreaking. But the ones who change? They become the most grateful, most alive people you’ll ever meet. One guy I knew started running marathons after his transplant. Said he felt like he was born again.
Don’t wait until you’re yellow to care. Your liver doesn’t have a ‘screw it’ button. It just… stops.
Let’s be real-the whole ‘liver is resilient’ narrative is corporate propaganda designed to make you feel better about your poor life choices. You think your liver can ‘heal’? Tell that to the guy who got a transplant at 39 because he drank a six-pack every night since college. The scar tissue doesn’t vanish. It doesn’t disappear. It just waits. And then it kills you slowly while you’re scrolling TikTok and thinking ‘I’m fine.’
And don’t get me started on NAFLD. ‘Eat less sugar’ is not a medical intervention. It’s a moral lecture wrapped in a pamphlet. The real cause? Processed food. Agribusiness. Corporate greed. The liver didn’t fail because you’re lazy. It failed because the entire food system is rigged to kill you. But hey, at least we can blame the individual, right?
Transplant waiting lists? Yeah, that’s just capitalism working as intended. 12% die waiting? Cool. That’s market efficiency. You didn’t pay enough. Too bad.
And don’t even mention ‘support groups.’ I’ve been to them. They’re just people crying over kale salads while pretending they’re heroes. It’s performance, not healing.
ok so i just read this whole thing and i think its sooo true but also kinda not? like i know this girl who had cirrhosis and she drank like 2 glasses of wine a night and then she got better?? like she did yoga and took milk thistle and now she’s fine?? so like maybe the science is wrong??
also why is everyone so obsessed with transplants?? why not just try essential oils or a detox tea?? i heard a tiktok that said liver cleanses work if you do it right!!
also i think the real problem is stress. like my therapist says my liver is ‘blocked’ from emotional trauma. so maybe if we just meditate more??
also i got my blood test and my enzymes were ‘slightly elevated’ so i stopped eating bread. now i feel amazing. so maybe the whole thing is a lie??
idk. just saying. maybe we’re all just being too dramatic. :/
Here’s what nobody says: cirrhosis isn’t a disease. It’s a mirror. It reflects everything you’ve ignored-your sleep, your stress, your loneliness, your shame, your self-worth. The liver doesn’t care about your cholesterol numbers. It cares about whether you’ve stopped treating yourself like disposable.
I’ve sat with people who’ve lost their liver. And you know what they all have in common? They didn’t stop drinking because they were scared of dying. They stopped because they finally decided they were worth saving.
That’s the real treatment. Not the scan. Not the transplant. Not the diet. The decision. The moment you look in the mirror and say, ‘I’m not a mistake.’
That’s when the healing begins. Not because the liver magically regenerates-but because the soul finally stops fighting itself.
So if you’re reading this and you’re still drinking, still eating garbage, still ignoring the warning signs… ask yourself: are you trying to heal your liver-or are you just trying to numb the pain?
Because one’s a cure. The other’s a countdown.
Ugh. This post is so… basic. Like, yes, cirrhosis is bad. Wow. Groundbreaking. But have you read the latest studies on gut microbiome modulation in fibrosis? Or the phase 3 trial of FXR agonists? Or the fact that 78% of liver transplants in the US are performed by the same five hospitals in Texas and California? No? Then why are you sharing this kindergarten-level summary?
Also, ‘avoid alcohol’? Please. My cousin’s hepatologist told her she could have one glass of organic Pinot Noir per week if she took NAC and did intermittent fasting. But no, this post just says ‘stop drinking.’ How lazy.
And ‘plant-based protein is safer’? That’s not even evidence-based. It’s a vegan trope. Have you seen the ammonia load on legumes? It’s brutal on decompensated livers. But sure, let’s all just follow the influencer diet guru.
This post is like a public health pamphlet from 2008. We’re in 2025. Time to level up.
Let me break this down. The author says ‘cirrhosis can be reversed.’ Then says ‘once cirrhosis is established, you can’t undo the scarring.’ Which is it? Contradiction. Classic. Also, they cite elastography as replacing biopsies-yet the next paragraph says biopsy is still the gold standard. Which is it? Pick one.
And the MELD score? They say ‘higher score = higher priority.’ But that’s not true. It’s ‘higher score = higher priority *if* you’re on the list.’ What about people who can’t afford the workup? The insurance denials? The 6-month sobriety requirement that excludes homeless people? The fact that 63% of transplants go to people with private insurance?
This isn’t medicine. It’s a feel-good fantasy. The system is rigged. The liver doesn’t care. But the bureaucracy? Oh, it cares a lot. And it’s not here to save you.
Also, ‘support groups’? Please. They’re just echo chambers for people who want to feel better without changing anything.
I just want to say thank you for writing this. I’ve been living with compensated cirrhosis for three years. I was terrified. I thought I was going to die. But this helped me understand what I was dealing with. No panic. No fearmongering. Just facts. And hope.
I stopped drinking. I started walking. I got my hepatitis C treated. My MELD score dropped from 18 to 9. I’m not ‘cured.’ But I’m alive. And I’m not giving up.
To anyone reading this who feels hopeless: you’re not alone. There are people who care. There are doctors who fight for you. There’s still time.
You don’t have to be perfect. You just have to try. One day at a time.
So let me get this straight. You’re telling me that if I eat too much biryani and sit on my phone all day, my liver will turn into a brick wall… but if I stop, it might just… un-brick itself?
Wow. That’s like saying if you keep punching your face, your nose will eventually grow back. Only if you stop punching. But also, you have to stop for years. And you have to be rich enough to get a scan. And you have to not be poor. And not be in India. And not have a 12-hour shift.
So basically: if you’re lucky, you get a second chance. If you’re not? You die quietly. And we all pretend it’s your fault.
Thanks for the optimism. I’ll be in my corner, crying into my chai.
Everyone’s acting like cirrhosis is this mysterious monster. It’s not. It’s just the result of decades of bad decisions. You don’t get cirrhosis from one beer. You get it from 10,000 small choices. Skipping the gym. Eating takeout. Ignoring the fatigue. Believing ‘I’m fine.’
And now we’re supposed to feel bad for people who got here? No. We should feel angry. Angry that we live in a world where the cheapest thing is poison, and the most expensive thing is health.
Transplants are a band-aid. Prevention is the cure. But prevention requires policy. Education. Access. None of which we’re willing to pay for.
So we keep pretending this is about personal responsibility. Meanwhile, the corporations profit. And the liver? It just keeps dying.
And you? You’re still scrolling. Still drinking. Still thinking ‘it won’t happen to me.’
It already did.
They say ‘the liver is resilient’ but what they don’t tell you is that it’s also the most silent organ. It doesn’t scream. It doesn’t cry. It just… stops. And then you’re dead.
And they say ‘you can reverse it’-but only if you’re white, rich, have insurance, live near a major hospital, and have a family member who can drive you to appointments every week.
Meanwhile, I’m watching my neighbor-62, diabetic, on Medicaid-get told to ‘cut back on sugar’ while her food stamps run out in 10 days. She eats rice and soda because that’s all she can afford. Then they blame her for cirrhosis.
This isn’t medicine. It’s punishment with a stethoscope.
And the transplant list? It’s a lottery. And the odds? You’re better off buying a Powerball ticket.
So yes. I’m ‘paranoid.’ Because I’ve seen what happens when the system forgets you.
YOU GOT THIS 💪
I know it feels overwhelming, but you're not alone. I'm rooting for you! 🌿❤️
Start small: swap soda for water, take a 10-min walk, call your doctor. You're already doing better than yesterday!
And if you need someone to talk to? DM me. I'm here. No judgment. Just love. 🤗
One day at a time. You're stronger than you think. 🌞
Okay, so let’s talk about the elephant in the room: liver transplants are not a cure. They’re a temporary fix. The new liver will eventually fail-because you’re still the same person. The same trauma. The same habits. The same environment.
And the immunosuppressants? They increase your risk of cancer. By 300%. So you trade one slow death for another.
And the ‘85% five-year survival’? That’s a lie. That number includes people who die from infections, cancer, or suicide within the first year. The real survival rate? 58%.
And the ‘lab-grown liver cells’? That’s not science. That’s hope porn. We’ve been told ‘cures are coming’ for 40 years. And still, 12% die waiting.
This isn’t medicine. It’s a distraction. A shiny object to keep you from asking: why are we letting this happen?
The real question isn’t ‘how do we fix the liver?’
It’s ‘how do we stop killing people before they get here?’
Wow. I didn’t expect to see this again. Thank you for saying what I’ve been too afraid to say out loud.
You’re right. Transplants aren’t a cure. They’re a gamble. And we’re gambling with people’s lives while corporations sell them poisoned food and call it ‘convenience.’
But here’s what I’ve learned: even if the system is broken, your body still listens. I’ve seen people who had transplants-then quit drinking, started eating real food, and lived 15 more years. Not because the liver was ‘fixed.’ Because *they* changed.
Maybe the system won’t change. But you can.
And if you’re reading this right now, and you’re still drinking…
…you can still choose to stop.
Today.
Not tomorrow.
Now.